Fill Out a Valid Nj Direct Claim Template
Navigating the complexities of health insurance claims can often feel like a daunting task, but the NJ Direct Claim Form is designed to streamline the process for members of the State Health Benefits Program (SHBP) and School Employees’ Health Benefits Program (SEHBP). This form, easily accessible for download from the Horizon Blue website, simplifies the submission of medical expenses by guiding subscribers through each step of providing necessary information. From noting the subscriber and patient details, including their employment and educational status, to specifying whether the claim is related to employment, an auto accident, or other incidents, the form ensures that all pertinent data is collected efficiently. It also addresses coordination with other health insurance coverage, providing a section for details on any additional health coverage plans. Notably, the form includes clear instructions for including medical diagnosis and itemized bills, highlighting the importance of attaching readable and complete documentation for every service or supply charged. Moreover, it elucidates the protocols for submitting claims when Medicare is involved, ensuring that those who are eligible can navigate their secondary NJ DIRECT coverage with ease. Importantly, the form concludes with an authorization section, underscoring the need for accuracy and honesty in claim submissions and signaling the potential legal consequences of fraudulent claims. By fulfilling these requirements, subscribers pave the way for a smoother claims process, reinforcing the importance of careful and comprehensive documentation in managing healthcare benefits.
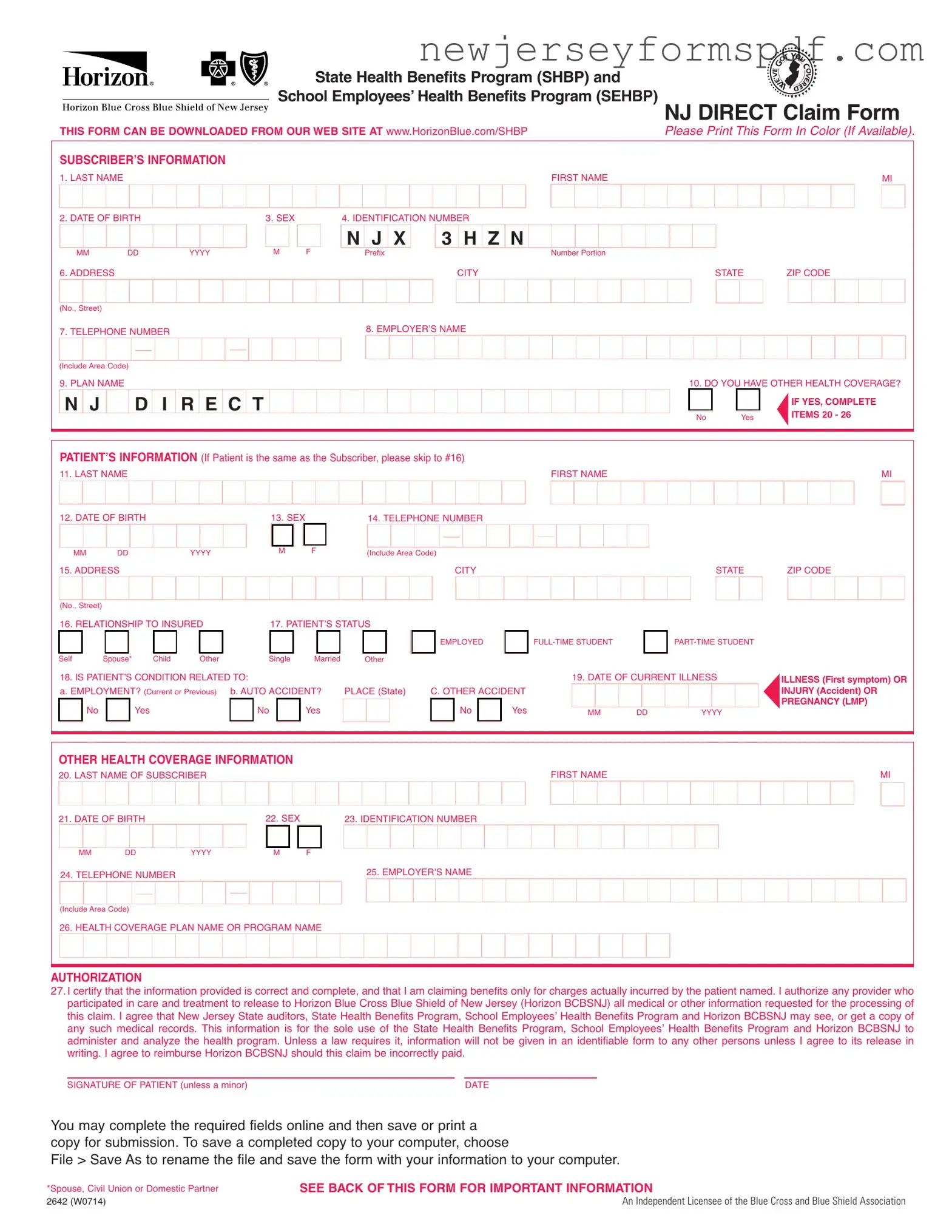
Sample - Nj Direct Claim Form
State Health Benefits Program (SHBP) and
School Employees’ Health Benefits Program(SEHBP)
THIS FORM CAN BE DOWNLOADED FROM OUR WEB SITE AT www.HorizonBlue.com/SHBP |
NJ DIRECT Claim Form |
Please Print This Form In Color (If Available). |
SUBSCRIBER’S INFORMATION |
|
|
|
|
|
FIRST NAME |
|
MI |
|||
1. LAST NAME |
|
|
|
|
|
|
|
|
|
||
2. DATE OF BIRTH |
|
|
3. SEX |
|
4. IDENTIFICATION NUMBER |
|
|
|
|
||
MM |
DD |
|
YYYY |
M |
F |
N J X |
3 H Z |
N |
Number Portion |
|
|
|
Prefix |
CITY |
|
STATE |
ZIP CODE |
||||||
6. ADDRESS |
|
|
|
|
|
|
|
|
|||
(No., Street) |
|
|
|
|
|
8. EMPLOYER’S NAME |
|
|
|
|
|
7. TELEPHONE NUMBER |
|
|
|
|
|
|
|
||||
(Include Area Code) |
|
|
|
|
|
|
|
10. DO YOU HAVE OTHER HEALTH COVERAGE? |
|||
9. PLAN NAME |
|
|
R E C T |
|
|
|
|
|
|||
N J |
D |
I |
|
|
|
|
|
No |
Yes |
IF YES, COMPLETE |
|
|
|
|
|
|
ITEMS 20 - 26 |
||||||
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
||
PATIENT’S INFORMATION (If Patient is the same as the Subscriber, please skip to #16) |
FIRST NAME |
MI |
||
11. LAST NAME |
|
|
||
12. DATE OF BIRTH |
13. SEX |
14. TELEPHONE NUMBER |
|
|
MM |
DD |
YYYY |
M |
F |
(Include Area Code) |
CITY |
STATE |
15. ADDRESS |
|
|
|
|
|||
ZIP CODE
(No., Street)
16. RELATIONSHIP TO INSURED
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
EMPLOYED |
|
||
|
Self |
|
|
Spouse* |
|
|
Child |
|
Other |
|
|
|
Single |
|
|
Married |
|
|
Other |
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
18. IS PATIENT’S CONDITION RELATED TO: |
|
|
|
|
PLACE (State) |
|
C. OTHER ACCIDENT |
||||||||||||||||||||
|
a. EMPLOYMENT? (Current or Previous) |
|
b. AUTO ACCIDENT? |
|
||||||||||||||||||||||||
|
|
No |
|
|
|
Yes |
|
|
|
|
No |
|
|
Yes |
|
|
|
|
|
|
|
No |
|
Yes |
||||
|
||
|
||
|
|
|
19.DATE OF CURRENT ILLNESS
MM DD 
 YYYY
YYYY
ILLNESS (First symptom) OR INJURY (Accident) OR PREGNANCY (LMP)
OTHER HEALTH COVERAGE INFORMATION |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
FIRST NAME |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
MI |
|||||||||||||||||||||||
20. LAST NAME OF SUBSCRIBER |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
21. DATE OF BIRTH |
|
|
|
|
22. SEX |
|
|
|
|
23. IDENTIFICATION NUMBER |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||||||
|
|
MM |
|
DD |
|
YYYY |
|
|
M |
|
|
|
F |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
25. EMPLOYER’S NAME |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||||||||||||
|
|
24. TELEPHONE NUMBER |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||||||||||
(Include Area Code)
26. HEALTH COVERAGE PLAN NAME OR PROGRAM NAME
27AUTHORIZATION.I certify that the information provided is correct and complete, and that I am claiming benefits only for charges actually incurred by the patient named. I authorize any provider who participated in care and treatment to release to Horizon Blue Cross Blue Shield of New Jersey (Horizon BCBSNJ) all medical or other information requested for the processing of this claim. I agree that New Jersey State auditors, State Health Benefits Program, School Employees’ Health Benefits Program and Horizon BCBSNJ may see, or get a copy of any such medical records. This information is for the sole use of the State Health Benefits Program, School Employees’ Health Benefits Program and Horizon BCBSNJ to administer and analyze the health program. Unless a law requires it, information will not be given in an identifiable form to any other persons unless I agree to its release in writing. I agree to reimburse Horizon BCBSNJ should this claim be incorrectly paid.
SIGNATURE OF PATIENT (unless a minor)DATE
You may complete the required fields online and then save or print a copy for submission. To save a completed copy to your computer, choose
File > Save As to rename the file and save the form with your information to your computer.
*Spouse, Civil Union or Domestic Partner |
SEE BACK OF THIS FORM FOR IMPORTANT INFORMATION |
2642 (W0714) |
An Independent Licensee of the Blue Cross and Blue Shield Association |
PLEASE READ THIS IMPORTANT INFORMATION
WHEN YOU ARE SUBMITTING EXPENSES FOR MORE THAN ONE FAMILY MEMBER, PLEASE USE A SEPARATE CLAIM FORM FOR EACH PERSON. ITEMIZED BILLS FOR COVERED SERVICES OR SUPPLIES MUST BE ATTACHED TO THIS FORM AND INCLUDE THE FOLLOWING:
Check that each itemized bill is legible and contains ALL of the following information:
☑ NAME & ADDRESS of person or institution rendering the service or supplying the item
☑ PATIENT’S FULL NAME
☑ TYPE of service rendered/produced or item supplied ☑ DATE each service rendered or item supplied
☑ AMOUNT charged for each service rendered or item supplied ☑ DIAGNOSIS of ailment
Cash register receipts, cancelled checks, money order receipts, personal itemizations, and bills only noting a "balance due" are not acceptable.
COORDINATION OF BENEFITS?
If you or your covered dependent(s) are covered by another health insurance program, please provide the information requested in the Other Health Coverage Section. Example: Spouse covered by another insurance company or other Horizon Blue Cross Blue Shield of New Jersey coverage.
When submitting charges for services or supplies that have been partially paid or declined by other group health coverage, attach a copy of the Notice of Payment or Explanation of Benefits from the other health care insurer along with itemized bill(s).
MEDICARE?
If PATIENTis eligible for Medicare Benefits, be sure you include the Explanation of Medicare Benefits (EOMB) that was sent to patient explaining the charges paid or not paid by Medicare.
To process a claim for your NJ DIRECT secondary coverage, we need a copy of the EOMB. This EOMB should have been sent to you when Medicare processed your claim. If your EOMB has more than one page, send us copies of all pages. Please write your NJ DIRECT identification number clearly on the first page.
CLAIM FORM MAY BE RETURNED TO YOU IF THIS ADDITIONAL INFORMATION IS NOT SUPPLIED
HELPFUL HINTS
When you are submitting expenses for more than one family member, please use a separate claim form for each person. It is suggested that you make copies for your own use before you submit the original bills.
Durable medical equipment? (Wheel chair, crutches, braces, oxygen, etc.) Your doctor’s certification must be submitted indicating the expected length of time the equipment will be in use. If renting, please have your medical equipment supplier also indicate the purchase price of the equipment on the bill. Foreign Claim? Bills for services incurred outside of the U.S. must include an English translation and the exchange rate at the time of services.
If you have any questions about how to submit your Claims, please call the Customer Service #
WHERE TO SUBMIT YOUR CLAIM FORMS
Please mail completed claim form for:
MEDICALHorizonCLAIMSBlue CrossTO:Blue Shield of New Jersey
P.O. Box 820
Newark, NJ
MENTALHorizonHEALTH/SUBSTANCEABUSEBlue Cross Blue Shield of NewCLAIMSJersey TO:
Horizon Behavioral Health
P.O. Box 10191
Newark, NJ
ANY PERSON WHO KNOWINGLY FILESFRAUDA STATEMENTWARNINGOF CLAIM CONTAINING ANY FALSE OR
MISLEADING INFORMATION IS SUBJECT TO CRIMINAL AND CIVIL PENALTIES
TO REPORT SUSPECTED FRAUD CALL
Document Specifications
| Fact Name | Description |
|---|---|
| Form Usage | This form is used for claims under the State Health Benefits Program (SHBP) and School Employees’ Health Benefits Program (SEHBP) in New Jersey. |
| Availability | The NJ DIRECT Claim Form can be downloaded from the Horizon Blue Cross Blue Shield of New Jersey website. |
| Submission Instructions | Itemized bills for covered services or supplies must be attached to the form, and each family member's expenses require a separate claim form. |
| Coordination of Benefits | Information about other health coverage must be provided, especially if the patient or dependents are covered under another insurance program. |
| Legal Implications | Submitting a claim with false or misleading information can result in criminal and civil penalties, as per the fraud warning on the form. |
| Governing Law | The form is governed by New Jersey state laws, specifically related to the State Health Benefits Program and School Employees’ Health Benefits Program. |
Detailed Steps for Using Nj Direct Claim
After completing the NJ Direct Claim form, it marks the beginning of the claim process for expenses incurred that might not have been covered initially. Each section of the form must be filled out carefully and accurately to ensure a smooth process. It is essential to attach all required documentation, such as itemized bills and, if applicable, other health coverage statements. Once the form and all attachments are prepared, they should be mailed to the specific address provided for either medical or mental health/substance abuse claims, depending on the nature of the expenses. The process following submission includes the review and processing of the claim by Horizon Blue Cross Blue Shield of New Jersey, which may involve additional communication for clarification or further information.
- Go to www.HorizonBlue.com/SHBP and download the NJ DIRECT Claim Form. If available, print the form in color.
- Fill in the SUBSCRIBER’S INFORMATION section starting with the subscriber's first name, middle initial, and last name.
- Enter the subscriber's Date of Birth as MM DD YYYY, select the Sex, and provide the Identification Number including prefix.
- Input the subscriber's address; include the city, state, and ZIP code.
- Add the subscriber's telephone number, including the area code.
- Specify the subscriber's Employer’s Name and Plan Name.
- If the subscriber has other health coverage, mark "Yes" and be prepared to complete items 20-26 related to the other health coverage.
- Move to the PATIENT’S INFORMATION section. If the patient is not the subscriber, enter their first name, middle initial, last name, date of birth, sex, telephone number, and address.
- Indicate the patient's Relationship to Insured and their Status (e.g., Employed, Single).
- Answer questions regarding if the patient’s condition is related to employment, an auto accident, or another accident, and specify the date of the current illness, injury, or pregnancy.
- For OTHER HEALTH COVERAGE INFORMATION, fill in the details of the subscriber of the other health plan, if applicable.
- In the authorization section at the bottom, review the certification statement, then have the patient or legal guardian sign and date the form to authorize the release of information and agreement with the statements provided.
- Ensure all necessary documents and itemized bills are attached.
- Mail the completed claim form and attachments to the corresponding address for either medical claims or mental health/substance abuse claims, as outlined in the instructions on where to submit your claim forms.
Remeber to keep a copy of all documents for your records before mailing. Accurate and complete submission aids in the timely processing of your claim.
Learn More on Nj Direct Claim
How do I submit a NJ Direct Claim form?
To submit a NJ Direct Claim form, first ensure that the form is filled out completely and accurately. Attach itemized bills for the covered services or supplies, which must include all of the required information such as the name and address of the service provider, patient’s full name, type of service or item supplied, date of service, charge amount, and the diagnosis. For expenses related to more than one family member, use a separate claim form for each person. If applicable, include a copy of the Notice of Payment or Explanation of Benefits from any other health care insurer or the Explanation of Medicare Benefits (EOMB) if the patient is eligible for Medicare Benefits. Mail the completed form and attachments to Horizon Blue Cross Blue Shield of New Jersey, P.O. Box 820, Newark, NJ 07101-0820 for medical claims or to Horizon Behavioral Health, P.O. Box 10191, Newark, NJ 07101-3189 for mental health/substance abuse claims.
What should I include with my NJ Direct Claim form?
- Itemized bills containing the provider’s name & address, patient's name, type of service/item, date of service, charge amount, and diagnosis.
- Notice of Payment or Explanation of Benefits from other insurers, if applicable.
- Explanation of Medicare Benefits (EOMB), if the patient is covered by Medicare.
- English translation and exchange rate for bills from services incurred outside of the U.S., if applicable.
What common mistakes should I avoid when filling out the NJ Direct Claim form?
Avoid the most common mistakes by double-checking the following before submission:
- Ensure all required fields are completed accurately.
- Attach all necessary documents, including itemized bills and any relevant notices of payment or benefits explanations.
- Use a separate claim form for each family member if submitting expenses for multiple people.
- Write the NJ DIRECT identification number clearly on all documents.
Where can I find more help with my NJ Direct Claim form?
If you need further assistance with your NJ Direct Claim form or have specific questions about the submission process, you can call the Customer Service number at 1-800-414-SHBP (7427). Representatives are available to help guide you through the process and answer any questions you may have.
Common mistakes
When individuals fill out the NJ Direct Claim form, common mistakes can lead to delays or denial of claims. Recognizing these pitfalls can streamline the submission process and facilitate quicker reimbursement. Below are eight notable errors often encountered.
- Failing to print the form in color when available, which aids in the clarity and readability of the information provided.
- Incorrectly entering the subscriber's identification number, a critical piece of data needed to match the claim to the correct policy.
- Omitting or inaccurately filling out the "Other Health Coverage" section, essential for coordinating benefits and ensuring proper payment.
- Not specifying the "Patient’s Relationship to Insured" accurately, which could misrepresent who the care was for and possibly affect coverage.
- Overlooking the need to attach itemized bills for each service or supply, providing crucial details of the claim.
- Submitting support documents without English translations and exchange rates for claims related to services outside of the U.S., necessary for proper processing.
- Forgetting to include the Explanation of Medicare Benefits (EOMB) when the patient is eligible for Medicare, a necessary step for those with secondary NJ Direct coverage.
- Not properly indicating whether the patient’s condition was related to employment, an auto accident, or another accident, information that is vital for correct liability assignment.
Avoiding these mistakes not only expedites the claim process but also helps ensure that individuals properly utilize their benefits. Mindful completion of the NJ Direct Claim form is crucial for a smooth, efficient claims experience.
Documents used along the form
When submitting a claim using the NJ Direct Claim Form for healthcare expenses under the State Health Benefits Program (SHBP) and School Employees’ Health Benefits Program (SEHBP), several other forms and documents may need to be attached or considered, depending on the specifics of the healthcare services provided and the circumstances of the patient. These additional documents play a critical role in ensuring the claim is processed efficiently and accurately.
- Itemized Bills: These documents should detail each service provided, including dates, charges, and provider information. They must be legible and contain comprehensive information to support the claim.
- Explanation of Benefits (EOB): Provided by the insurer, this document outlines what has been paid towards a claim and what the patient owes. It is necessary when coordinating benefits or if the primary insurer has partially paid for the services.
- Medicare Explanation of Medicare Benefits (EOMB): For patients eligible for Medicare, the EOMB shows charges paid or not paid by Medicare. It is essential for processing a claim when NJ DIRECT is the secondary coverage.
- Prescription Receipts: Detailed receipts from pharmacies are required for medications covered under the plan. These receipts include the patient's name, the prescription date, the medication dispensed, and the cost.
- Referral Forms: If the healthcare service requires a referral, the referral form from the primary care physician indicating the necessity of the specialized service must be attached.
- Accident Reports: If the claim involves an injury related to an auto accident or is work-related, official accident reports or a worker’s compensation notice may be required to determine liability and coverage.
- Doctor’s Certification for Durable Medical Equipment (DME): For claims involving durable medical equipment like wheelchairs or braces, a doctor’s certification indicating the necessity and expected duration of use is required. For rented equipment, the purchase price and rental agreement may also be needed.
Accurate and complete documentation is vital to the claims process, ensuring that benefits are correctly administered and that patients receive the reimbursements they are entitled to. Each of the documents listed above serves a specific purpose in conveying necessary information about the service provided, the context of the health condition being treated, and the financial aspects of the claim. Careful attention to the requirements for each document will assist in a smoother processing of healthcare claims.
Similar forms
The Health Insurance Claim Form, often recognized as the CMS-1500, is remarkably similar to the NJ Direct Claim Form. Both are designed to collect detailed information from patients, including personal, insurance, and medical service details. The key difference lies in their scope; while the CMS-1500 is widely used across various healthcare providers for insurance billing, the NJ Direct Claim Form is specifically tailored for members of the State Health Benefits Program (SHBP) and School Employees’ Health Benefits Program (SEHBP) in New Jersey. Yet, both serve the critical function of facilitating reimbursement for healthcare services.
The Universal Claim Form, used in pharmacy billing, shares similarities with the NJ Direct Claim Form in its purpose to facilitate the reimbursement process. However, it focuses on pharmaceutical services. Similar to the NJ Direct Claim Form, it requires patient information and specifics about the prescriber and the dispensed medication. The main objective is to ensure that patients or healthcare plan members can claim back expenses incurred for their prescriptions, mirroring the process for medical services claims.
Dental Claim Forms are used for submitting charges related to dental services, akin to how the NJ Direct Claim Form is utilized for health services. Both forms collect identification and procedural information to ensure appropriate processing and reimbursement by insurance companies. Although one is tailored to general health services and the other to dental care, their underlying purpose of detailing service costs for insurance purposes aligns them closely.
The Auto Insurance Claim Form, while varying in context—addressing vehicle accidents and related medical treatments—shares with the NJ Direct Claim Form the goal of acquiring compensation or coverage. They gather detailed information on the patient or claimant, the nature of the incident or ailment, and the costs involved. Despite the difference in the type of insurance, both forms facilitate claims processing to cover expenses arising from their respective incidents.
The Workers' Compensation Claim Form also mirrors the NJ Direct Claim Form in its core objective, though it specifically addresses injuries or illnesses acquired in the workplace. Both require detailed incident reporting and personal information to assess claims for compensation or medical cost coverage. The emphasis is on documenting the circumstances and health impact of work-related incidents versus general health conditions or treatments.
The Disability Claim Form, like the NJ Direct Claim Form, is essential for individuals seeking compensation due to illness or injury-related work inability. While one is broad in health service coverage, the latter specifically targets disability incidents, requiring detailed medical and personal information to evaluate eligibility for benefits. Both play pivotal roles in providing financial support during health-related work absences.
Medicare Claim Forms share a purpose with the NJ Direct Claim Form: ensuring that recipients are reimbursed for medical expenses. Although aimed at the senior population and specific others eligible for Medicare, the form requires similar comprehensive details about medical services received. Each form plays a critical role within its insurance structure, enabling healthcare services reimbursement.
The Health Care Flexible Spending Account (FSA) Reimbursement Form, paralleling the NJ Direct Claim Form, targets a different facet of healthcare financing. Utilized for claiming out-of-pocket healthcare expenses under an FSA, it seeks detailed billing information to process reimbursements, akin to insurance claims. Though one operates within a flexible spending account framework and the other within traditional insurance, their mutual goal is to facilitate coverage for health-related expenses.
The Long-Term Care Insurance Claim Form, while geared towards covering services like assisted living or home healthcare, aligns with the NJ Direct Claim Form in facilitating claims for covered services. Both demand comprehensive data on the care provided and its costs, underscoring the insurance mechanism's role in managing and reimbursing healthcare expenses. The focus on detailed documentation ensures that beneficiaries receive due benefits for their care needs.
Last, the Vision Care Claim Form is analogous to the NJ Direct Claim Form but centers on eye care services. Requiring details on the provider, services, and charges, it ensures that vision care expenses are meticulously documented for insurance reimbursement. Both forms serve as critical tools in their respective areas to enable patients to claim insurance benefits for healthcare services, thereby alleviating financial burdens tied to health and wellness maintenance.
Dos and Don'ts
When you're filling out the NJ Direct Claim Form for health benefits under the State Health Benefits Program (SHBP) or School Employees’ Health Benefits Program (SEHBP), the process can seem daunting. However, with a few guidelines in mind, you can complete this task confidently and accurately. Below are things you should and shouldn't do when completing the form:
- Do ensure all information provided is accurate and complete. Your claim's successful processing depends on the clarity and correctness of the details you submit.
- Don't leave mandatory fields empty. If a section applies to you or the patient, fill it in. Incomplete forms may lead to delays or rejection of your claim.
- Do attach itemized bills for covered services or supplies. Each bill should include the patient's full name, the date of service, the provider's name and address, the type of service, and the charge for each service.
- Don't submit illegible copies or documents with missing information. Bills lacking the required details might be returned to you, causing further delay.
- Do provide details of any other health coverage if applicable. The coordination of benefits is crucial to ensuring that your claim is processed smoothly.
- Don't forget to sign and date the form. Your signature verifies that the information provided is correct and complete, and it authorizes the release of medical or other information required for the processing of this claim.
- Do make copies of the claim form and attached bills for your records before submission. Keeping a record can be extremely helpful in case of discrepancies or queries.
- Don't hesitate to contact customer service if you have questions about how to submit your claim. It's better to get clarity beforehand than to have your claim returned or delayed.
By keeping these dos and don'ts in mind, you can navigate the process of submitting your NJ Direct Claim Form with greater ease and confidence, ensuring a smoother path to receiving the benefits you're entitled to.
Misconceptions
When dealing with the NJ Direct Claim form, understanding its purpose and requirements is crucial for a smooth process. However, there are common misconceptions that can complicate or delay claims. Here are five such misconceptions clarified:
- Printing in Color is Necessary: While the form suggests printing in color if available, it is not a mandate. The primary goal is legibility. Claims will not be denied solely because they are not in color. It's more important that all the required fields are completed accurately.
- One Claim Form per Family is Sufficient: Each family member’s expenses require a separate claim form. This helps in organizing and processing each claim efficiently. Mixing expenses for multiple family members on a single form can lead to processing delays or errors.
- Submission Without Itemized Bills is Adequate: Itemized bills are essential for the claims process. These documents provide detailed information about the services received, such as the date of service, the provider’s name and address, and the amount charged. Receipts that simply indicate a balance due or personal itemizations without specifics are not acceptable.
- All Sections Must be Completed for Every Submission: While thorough completion of the form is necessary, some sections may not apply to your situation, such as "Other Health Coverage" if the patient has no other insurance. It's important to read and fill out the form based on your specific circumstances. Overlooking sections that are not applicable to your situation will not invalidate your claim.
- Physical Submission is the Only Way: While the form gives an address for mailing, it does not preclude other methods of submission that Horizon BCBSNJ may offer, such as online submissions or electronic claims. It's always a good idea to check the most current process for submitting claims on their website or by contacting customer service.
Correcting these misconceptions can lead to a smoother, more efficient claims process, ensuring you get the benefits you’re entitled to without unnecessary delay. Always refer to the most recent guidelines provided by Horizon BCBSNJ to ensure compliance with their claims submission requirements.
Key takeaways
Filling out the NJ Direct Claim form correctly is crucial for timely and accurate processing of your health insurance claims. Here are five key takeaways to ensure that your claims are handled smoothly:
- Ensure Readability: Make sure all itemized bills are legible and contain the necessary information such as the service provider's name and address, patient's full name, type of service or item supplied, date of service or supply, amount charged, and diagnosis. This detail is essential for the claim to be processed.
- Separate Claims for Family Members: If you're submitting expenses for more than one family member, use a separate NJ Direct Claim form for each individual. This helps in organizing and expediting the claim process.
- Coordination of Benefits: If the patient or any of your dependents have other health coverage, make sure to fill out the section about other health coverage information. Include a copy of the Notice of Payment or Explanation of Benefits from the other insurer if applicable.
- Mandatory for Medicare Recipients: If the patient is eligible for Medicare Benefits, attach a copy of the Explanation of Medicare Benefits (EOMB) sent by Medicare. This document is crucial for processing your NJ DIRECT secondary coverage claim.
- Keep Copies: Before submitting the NJ Direct Claim form and any accompanying documents, it’s advisable to make copies for your records. This step ensures you have backup documentation in case the original materials are misplaced or there are disputes regarding the claim.
Remember, incomplete or incorrectly filled forms may result in delays or denials of the claim. Always review your form for accuracy and completeness before submission. Additionally, if you have any questions about how to submit your claim or require clarification on the form, contacting the customer service number provided on the form is recommended.
Popular PDF Documents
How to Get a Police Report Nj - This form helps businesses adhere to New Jersey's commitment to equal employment and non-discrimination.
Realtors Nj - Reminds sellers of their obligation to disclose any known material defects that could affect the property's value or safety.