Fill Out a Valid Nj Universal Physician Application Template
Navigating the complexities of healthcare documentation in New Jersey, the Universal Physician Application form serves as a crucial tool for physicians aiming to streamline their credentialing process. This comprehensive document covers a broad spectrum of personal and professional data, including, but not limited to, basic personal information, practice locations, and service types provided by the physician. It delves into intricate details like license information, certifications across various states, and even educational background, spanning from undergraduate degrees to post-graduate education and beyond. Furthermore, the form addresses professional and medical specialty information, detailing board certifications, preferred practice areas, and hospital affiliations, to ensure a thorough evaluation of the physician’s qualifications and areas of expertise. It also asks for a detailed work history, references, and information about professional liability insurance coverage, painting a complete picture of the physician’s professional journey. The inclusion of sections on outside interests and office coverage insights into the physician’s broader professional network and commitments. Designed with both clarity and comprehensiveness in mind, the New Jersey Universal Physician Application facilitates a smoother credentialing process, paving the way for physicians to focus more on patient care and less on bureaucratic hurdles.
Sample - Nj Universal Physician Application Form
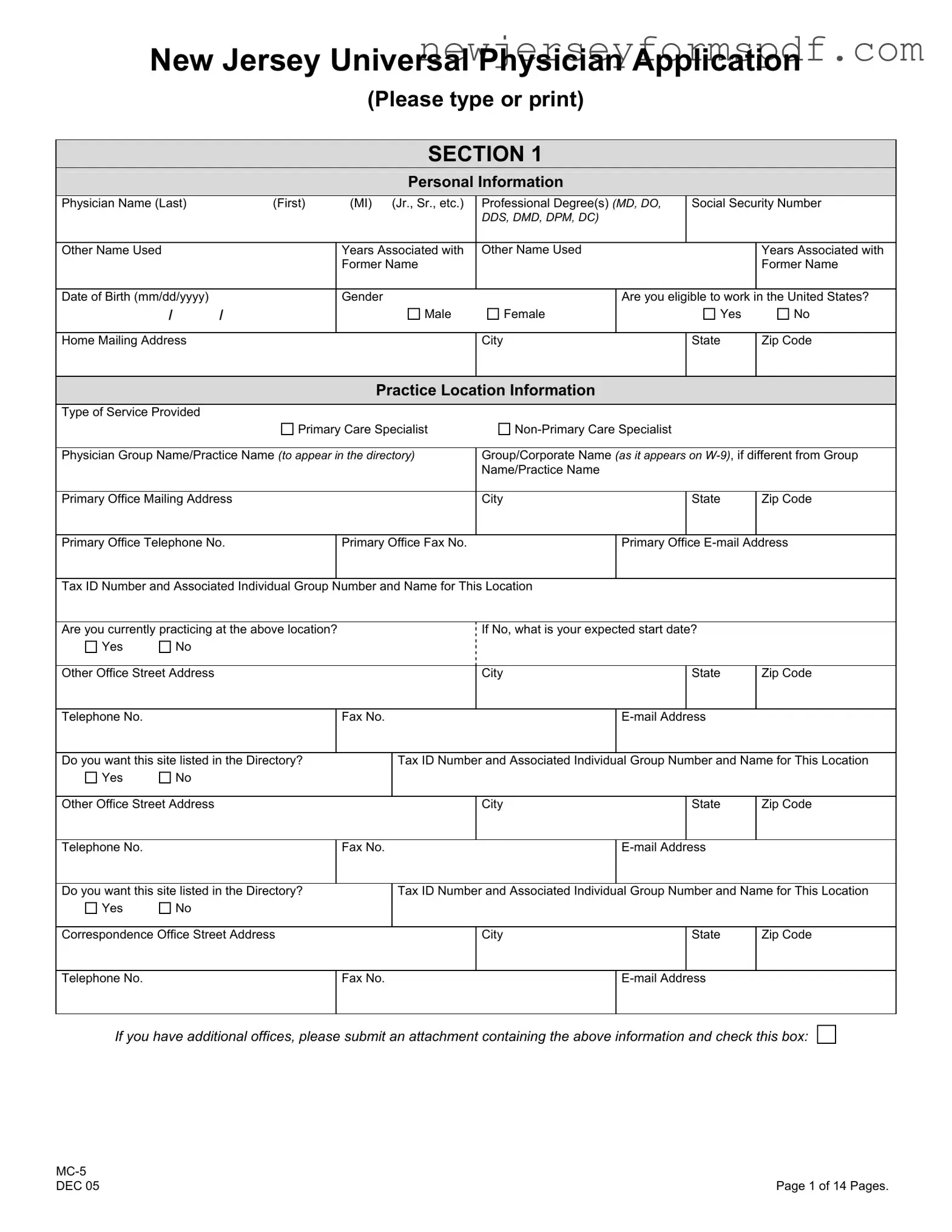
New Jersey Universal Physician Application
(Please type or print)
SECTION 1
Personal Information
Physician Name (Last) |
|
(First) |
(MI) (Jr., Sr., etc.) |
Professional Degree(s) (MD, DO, |
Social Security Number |
||
|
|
|
|
DDS, DMD, DPM, DC) |
|
|
|
|
|
|
|
|
|
|
|
Other Name Used |
|
|
Years Associated with |
Other Name Used |
|
Years Associated with |
|
|
|
|
Former Name |
|
|
|
Former Name |
|
|
|
|
|
|
|
|
Date of Birth (mm/dd/yyyy) |
|
|
Gender |
|
Are you eligible to work in the United States? |
||
/ |
/ |
|
Male |
Female |
|
Yes |
No |
|
|
|
|
|
|
|
|
Home Mailing Address |
|
|
|
City |
State |
Zip Code |
|
|
|
|
|
|
|
|
|
Practice Location Information
Type of Service Provided |
|
|
|
|
|
|
||
|
Primary Care Specialist |
|
||||||
|
|
|
|
|
|
|
||
Physician Group Name/Practice Name (to appear in the directory) |
Group/Corporate Name (as it appears on |
|||||||
|
|
|
|
|
Name/Practice Name |
|
|
|
|
|
|
|
|
|
|
|
|
Primary Office Mailing Address |
|
|
City |
|
State |
Zip Code |
||
|
|
|
|
|
|
|
|
|
Primary Office Telephone No. |
|
Primary Office Fax No. |
|
Primary Office |
||||
|
|
|
|
|
|
|||
Tax ID Number and Associated Individual Group Number and Name for This Location |
|
|
|
|||||
|
|
|
|
|
||||
Are you currently practicing at the above location? |
|
|
If No, what is your expected start date? |
|
||||
Yes |
No |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Other Office Street Address |
|
|
City |
|
State |
Zip Code |
||
|
|
|
|
|
|
|
|
|
Telephone No. |
|
|
Fax No. |
|
|
|||
|
|
|
|
|
||||
Do you want this site listed in the Directory? |
|
Tax ID Number and Associated Individual Group Number and Name for This Location |
||||||
Yes |
No |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Other Office Street Address |
|
|
City |
|
State |
Zip Code |
||
|
|
|
|
|
|
|
|
|
Telephone No. |
|
|
Fax No. |
|
|
|||
|
|
|
|
|
||||
Do you want this site listed in the Directory? |
|
Tax ID Number and Associated Individual Group Number and Name for This Location |
||||||
Yes |
No |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Correspondence Office Street Address |
|
|
City |
|
State |
Zip Code |
||
|
|
|
|
|
|
|
|
|
Telephone No. |
|
|
Fax No. |
|
|
|||
|
|
|
|
|
|
|
|
|
If you have additional offices, please submit an attachment containing the above information and check this box:
|
|
DEC 05 |
Page 1 of 14 Pages. |
NEW JERSEY UNIVERSAL PHYSICIAN APPLICATION (Continued)
License and Other Identification Numbers
(License Information - Include all license(s) and certifications in all States where you are currently or have previously been licensed.)
|
Type |
State(s) of |
|
Do You Currently |
License/Certificate |
|
Expiration |
|
N/A |
|||||
|
Registration |
|
Practice In This State? |
Number |
|
Date |
|
|||||||
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
License |
|
|
|
|
|
Yes |
No |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
License |
|
|
|
|
|
Yes |
No |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DEA Registration Certificate |
|
|
|
Yes |
No |
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CDS Registration Certificate |
|
|
|
Yes |
No |
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Other (CDS/DEA) (Specify) |
|
|
|
Yes |
No |
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
UPIN |
|
National Provider ID |
|
Are you a participating |
Medicare Provider No. |
Are you a participating |
Medicaid Provider No. |
|||||||
|
|
(when available) |
|
Medicare Provider? |
|
|
Medicaid Provider? |
|
|
|||||
|
|
|
|
|
|
|
|
|
||||||
International Medical Graduates: Are you certified by the Educational |
If yes, ECFMG Number |
|
ECFMG Issue Date |
|
||||||||||
Council for Foreign Medical Graduates (ECFMG)? |
|
|
|
|
|
|
|
|
|
|
||||
Yes |
No |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Medical Education
School Issuing Professional Degree (Medical, Dental, Chiropractic)
Degree
Attendance Dates
Address
City
State/Country
Zip Code
If you have attended additional schools, please submit an attachment containing the above information and check this box:
|
Institution Name |
|
|
|
Internship |
Fellowship |
|
|
|
Residency |
Teaching Appointment |
|
|
|
|
|
|
|
|
Address |
|
City |
State |
Zip Code |
|
|
|
|
|
Specialty |
|
Start Date (Month/Year) |
End Date (Month/Year) |
|
|
|
|
|
|
|
Institution Name |
|
|
|
Internship |
Fellowship |
|
|
|
Residency |
Teaching Appointment |
|
|
|
|
|
|
|
|
Address |
|
City |
State |
Zip Code |
|
|
|
|
|
Specialty |
|
Start Date (Month/Year) |
End Date (Month/Year) |
|
|
|
|
|
|
|
Institution Name |
|
|
|
Internship |
Fellowship |
|
|
|
Residency |
Teaching Appointment |
|
|
|
|
|
|
|
|
Address |
|
City |
State |
Zip Code |
|
|
|
|
|
Specialty |
|
Start Date (Month/Year) |
End Date (Month/Year) |
|
|
|
|
|
|
If you completed additional training, please submit an attachment containing the above information and check this box:
Other Graduate Level Education for Which a Degree Was Obtained - |
Institution Name |
|
|
|
Type of Program (Psychology, Public Health, MBA, etc.) |
|
|
|
|
|
|
|
|
|
Address |
City |
|
State |
Zip Code |
|
|
|
|
|
Degree Obtained |
|
Date of Graduation (Month/Year) |
||
|
|
|
|
|
|
|
DEC 05 |
Page 2 of 14 Pages. |
NEW JERSEY UNIVERSAL PHYSICIAN APPLICATION (Continued)
Professional/Medical Specialty Information
Primary Specialty |
|
|
Board Certified? |
|
Name of Certifying Board |
|
|||
|
|
|
Yes |
|
No |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Initial Certification Date |
|
|
Recertification Date (s) (if applicable) |
|
Expiration Date (if applicable) |
|
|||
|
|
|
|
|
|
||||
Do you wish to be listed in the directory under this specialty? |
If not Board Certified, indicate any of the following that apply: |
|
|||||||
HMO |
Yes |
No |
|
I have taken exam, results pending for: |
|
(board) |
|||
PPO |
Yes |
No |
|
I am intending to sit for the Boards on: |
|
(date) |
|||
POS |
Yes |
No |
|
I am not planning to take the Boards. |
|
||||
|
|
|
|
|
|
|
|
||
Secondary Specialty |
|
|
Board Certified? |
|
Name of Certifying Board |
|
|||
|
|
|
Yes |
|
No |
|
|
|
|
|
|
|
|
|
|
|
|||
Initial Certification Date |
|
|
Recertification Date (s) (if applicable) |
|
Expiration Date (if applicable) |
|
|||
|
|
|
|
|
|||||
Do you wish to be listed in the directory under this specialty? |
If not Board Certified, indicate any of the following that apply: |
|
|||||||
HMO |
Yes |
No |
|
I have taken exam, results pending for: |
|
(board) |
|||
PPO |
Yes |
No |
|
I am intending to sit for the Boards on: |
|
(date) |
|||
POS |
Yes |
No |
|
I am not planning to take the Boards. |
|
||||
|
|
|
|
|
|
|
|
||
Additional Specialty |
|
|
Board Certified? |
|
Name of Certifying Board |
|
|||
|
|
|
Yes |
|
No |
|
|
|
|
|
|
|
|
|
|
|
|||
Initial Certification Date |
|
|
Recertification Date (s) (if applicable) |
|
Expiration Date (if applicable) |
|
|||
|
|
|
|
|
|||||
Do you wish to be listed in the directory under this specialty? |
If not Board Certified, indicate any of the following that apply: |
|
|||||||
HMO |
Yes |
No |
|
I have taken exam, results pending for: |
|
(board) |
|||
PPO |
Yes |
No |
|
I am intending to sit for the Boards on: |
|
(date) |
|||
POS |
Yes |
No |
|
I am not planning to take the Boards. |
|
||||
|
|
|
|
|
|
|
|
|
|
List Additional Areas of Professional Practice, Interest or Focus (HIV/AIDS, etc.)
Hospital Affiliations and Privileges
Do you have hospital privileges? |
|
If you do not admit patients, what admitting arrangements do you have? |
|
|
|||
Yes |
No |
|
|
|
|
|
|
If you have privileges, please complete the section below. Include all hospitals where you have privileges.
Primary Hospital where you have Admitting Privileges |
|
|
Telephone Number |
|
||||
|
|
|
|
|
|
|
|
|
Address |
|
|
City |
|
|
|
State |
Zip Code |
|
|
|
|
|
|
|
||
Full Unrestricted Privileges |
Type of Privileges |
Are Privileges Temporary? |
|
Of the total admissions to all hospitals in the |
||||
Yes |
No |
|
Yes |
No |
|
past year, what percentage is to this specific |
||
|
|
|
|
|
||||
|
|
|
|
|
|
hospital? |
|
|
Other Hospital Where you Have Privileges |
|
|
Telephone Number |
|
||||
|
|
|
|
|
|
|
|
|
Address |
|
|
City |
|
|
|
State |
Zip Code |
|
|
|
|
|
|
|
||
Full Unrestricted Privileges |
Type of Privileges |
Are Privileges Temporary? |
|
Of the total admissions to all hospitals in the |
||||
Yes |
No |
|
Yes |
No |
|
past year, what percentage is to this specific |
||
|
|
|
|
|
||||
|
|
|
|
|
|
hospital? |
|
|
Other Hospital Where you Have Privileges |
|
|
Telephone Number |
|
||||
|
|
|
|
|
|
|
|
|
Address |
|
|
City |
|
|
|
State |
Zip Code |
|
|
|
|
|
|
|
||
Full Unrestricted Privileges |
Type of Privileges |
Are Privileges Temporary? |
|
Of the total admissions to all hospitals in the |
||||
Yes |
No |
|
Yes |
No |
|
past year, what percentage is to this specific |
||
|
|
|
|
|
||||
|
|
|
|
|
|
hospital? |
|
|
Additional Hospital Where you Have Privileges |
|
|
Telephone Number |
|
||||
|
|
|
|
|
|
|
|
|
Address |
|
|
City |
|
|
|
State |
Zip Code |
|
|
|
|
|
|
|
||
Full Unrestricted Privileges |
Type of Privileges |
Are Privileges Temporary? |
|
Of the total admissions to all hospitals in the |
||||
Yes |
No |
|
Yes |
No |
|
past year, what percentage is to this specific |
||
|
|
|
|
|
||||
|
|
|
|
|
|
hospital? |
|
|
If you have additional hospital affiliations, please submit an attachment containing the above information and check this box:
|
|
DEC 05 |
Page 3 of 14 Pages. |
NEW JERSEY UNIVERSAL PHYSICIAN APPLICATION (Continued)
List all other hospitals where you have previously had privileges.
Hospital Name
Dates of Affiliation
Address
City
State
Zip Code
Hospital Name
Dates of Affiliation
Address
City
State
Zip Code
If you have other previous hospital affiliations, please submit an attachment containing the above information and check this box:
Work History
Include chronological work history since completion of training.
Practice/Employer Name
Start Date/End Date
Address
City
State
Zip Code
Practice/Employer Name
Start Date/End Date
Address
City
State
Zip Code
Practice/Employer Name
Start Date/End Date
Address
City
State
Zip Code
Practice/Employer Name
Start Date/End Date
Address
City
State
Zip Code
For additional work history, please submit an attachment containing the above information and check this box:
Please provide an explanation of any gaps greater than six months in each work history.
Date
Explanation
Date
Explanation
Are you currently on active military duty or on military reserve?
Yes
No
References
Please provide three professional references that are not partners in your own group practice and are not relatives.
Name
Street Address
City, State, Zip Code
|
|
DEC 05 |
Page 4 of 14 Pages. |
NEW JERSEY UNIVERSAL PHYSICIAN APPLICATION (Continued)
Professional Liability Insurance Coverage
Are you |
|
|
|
|
|
|
|
|
|
|
Yes |
No |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Name of Current Malpractice Insurance Carrier or |
|
Telephone Number |
Effective Date |
Expiration Date |
|||||
|
|
|
|
|
|
|
|
|
|
Address |
|
|
|
|
City |
|
|
State |
Zip Code |
|
|
|
|
|
|
|
|
||
Policy Number |
Amount of Coverage per Occurrence |
|
Amount of Coverage Aggregate |
Type of Coverage |
Length of Time with |
||||
|
|
|
|
|
|
|
Individual |
Carrier |
|
|
|
|
|
|
|
|
Shared |
|
|
Name of Previous Malpractice Insurance Carrier or |
|
Telephone Number |
Effective Date |
Expiration Date |
|||||
|
|
|
|
|
|
|
|
|
|
Address |
|
|
|
|
City |
|
|
State |
Zip Code |
|
|
|
|
|
|
|
|||
Policy Number |
Amount of Coverage per Occurrence |
|
Amount of Coverage Aggregate |
Type of Coverage |
Length of Time with |
||||
|
|
|
|
|
|
|
Individual |
Carrier |
|
|
|
|
|
|
|
|
Shared |
|
|
Status/Role in Practice
Owner |
Partner |
Employee |
Officer |
Shareholder |
Interests in Outside Clinical Lab(s)
If you
Legal Billing Name |
TIN (Attach copy of |
Clinical Description |
|
|
|
Please provide a summary pattern for this business: |
|
|
Office Coverage |
|
|
List names of colleague(s) providing regular coverage and his/her specialty(ies). |
|
|
Name |
|
Provider Specialty |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Partners |
|
|
List full names of all partners in your practice (attach list for large group). |
|
|
Name (Last, First, MI) |
|
Name (Last, First, MI) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
DEC 05 |
Page 5 of 14 Pages. |
NEW JERSEY UNIVERSAL PHYSICIAN APPLICATION (Continued)
Other Practice Information (specify for each site)
|
|
|
|
|
|
|
|
Site 1 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Site 2 |
|
|
|
|
|
|
||||
Office Address: |
|
|
|
|
|
|
|
|
|
|
|
Office Address: |
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
Type of Practice: |
|
|
|
|
|
|
|
|
|
|
|
Type of Practice: |
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
Solo |
|
|
Single Specialty Group |
|
Solo |
|
|
Single Specialty Group |
|||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
Office Manager or Business Office Staff Contact:: |
|
|
|
|
Office Manager or Business Office Staff Contact:: |
|
|
|
||||||||||||||||||||||||||
|
Name: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Name: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
Telephone No.: |
|
|
|
|
|
|
|
|
|
|
|
|
Telephone No.: |
|
|
|
|
|
|
|
|
|
|
||||||||||
|
Fax No.: |
|
|
|
|
|
|
|
|
|
|
|
|
|
Fax No.: |
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
Credentialing Contact (if different from above): |
|
|
|
|
Credentialing Contact (if different from above): |
|
|
|
||||||||||||||||||||||||||
|
Name: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Name: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
Telephone No.: |
|
|
|
|
|
|
|
|
|
|
|
|
Telephone No.: |
|
|
|
|
|
|
|
|
|
|
||||||||||
|
Fax No.: |
|
|
|
|
|
|
|
|
|
|
|
|
|
Fax No.: |
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
Address: |
|
|
|
|
|
|
|
|
|
|
|
|
Address: |
|
|
|
|
|
|
|
|
|
|
||||||||||
|
City: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
City: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
State: |
|
|
|
|
|
|
|
|
|
Zip: |
|
|
|
|
|
|
State: |
|
|
|
|
|
|
|
|
|
Zip: |
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
Billing Information: |
|
|
|
|
|
|
|
|
|
|
|
Billing Information: |
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
Billing Rep. Name: |
|
|
|
|
|
|
|
|
Billing Rep. Name: |
|
|
|
|
|
|
||||||||||||||||||
|
Address: |
|
|
|
|
|
|
|
|
|
|
|
|
Address: |
|
|
|
|
|
|
|
|
|
|
||||||||||
|
City: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
City: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
State: |
|
|
|
|
|
|
|
|
|
Zip: |
|
|
|
|
|
State: |
|
|
|
|
|
|
|
|
|
Zip: |
|
|
|
|
|||
|
Telephone No.: |
|
|
|
|
|
|
|
|
|
|
|
|
Telephone No.: |
|
|
|
|
|
|
|
|
|
|
||||||||||
|
Fax No.: |
|
|
|
|
|
|
|
|
|
|
|
|
|
Fax No.: |
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
Dept. Name if |
|
|
|
|
|
|
|
|
|
Dept. Name if |
|
|
|
|
|
|
|
||||||||||||||||
|
Check should be payable to |
|
|
|
|
|
|
|
|
Check should be payable to |
|
|
|
|
|
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||
|
Do you have capability of electronic billing? |
Yes |
No |
|
Do you have capability of electronic billing? |
Yes |
No |
|||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||
Office Business Hours (hours patients are seen): |
|
|
|
|
Office Business Hours (hours patients are seen): |
|
|
|
||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
No |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
No |
|
|
|
|
|
|
|
|
|
|
|
||
Day |
|
Office |
|
Morning |
|
Afternoon |
Evening |
Day |
|
Office |
|
Morning |
|
Afternoon |
Evening |
|||||||||||||||||||
|
|
|
Hours |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Hours |
|
|
|
|
|
|
|
|
|
|
|
||||
MON |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
MON |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
TUES |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
TUES |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
WED |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
WED |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
THUR |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
THUR |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
FRI |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
FRI |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
SAT |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
SAT |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
SUN |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
SUN |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
After hours, back office phone number |
|
|
|
|
|
|
After hours, back office phone number |
|
|
|
|
|
||||||||||||||||||||||
for health plan business use only: |
|
|
|
|
|
|
|
for health plan business use only: |
|
|
|
|
|
|
||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||||||
Do you provide 24 hour/7 day a |
|
|
|
|
|
|
|
Do you provide 24 hour/7 day a |
|
|
|
|
|
|
||||||||||||||||||||
week phone coverage for this site? |
|
Yes |
No |
|
|
|
week phone coverage for this site? |
|
Yes |
No |
|
|
||||||||||||||||||||||
|
If yes, indicate type: |
|
|
|
|
|
|
|
|
If yes, indicate type: |
|
|
|
|
|
|
||||||||||||||||||
|
Answering service |
|
|
|
|
|
|
|
|
Answering service |
|
|
|
|
|
|
||||||||||||||||||
|
Voice mail with instructions to call answering service |
|
|
|
|
Voice mail with instructions to call answering service |
|
|
||||||||||||||||||||||||||
|
Voice mail with other instructions |
|
|
|
|
|
|
|
Voice mail with other instructions |
|
|
|
|
|
||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(Continue on next page.)
|
|
DEC 05 |
Page 6 of 14 Pages. |
NEW JERSEY UNIVERSAL PHYSICIAN APPLICATION (Continued)
Other Practice Information (specify for each site)
(Continued from previous page.)
|
|
|
|
Site 1, Continued |
|
|
|
|
|
|
|
|
|
Site 2, Continued |
|
|
|
|
|
||||||
Do you accept new patients into the practice? |
Yes |
No |
Do you accept new patients into the practice? |
Yes |
No |
||||||||||||||||||||
|
|
|
|
|
Yes |
No |
|
|
|
|
|
Yes |
No |
||||||||||||
|
Yes |
No |
|
Yes |
No |
||||||||||||||||||||
|
Yes |
No |
|
Yes |
No |
||||||||||||||||||||
|
|
Yes |
No |
|
|
Yes |
No |
||||||||||||||||||
|
|
Yes |
No |
|
|
Yes |
No |
||||||||||||||||||
If this information varies by health plan, provide explanation: |
If this information varies by health plan, provide explanation: |
||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
Are there any practice limitations? |
Yes |
|
|
No |
|
|
Are there any practice limitations? |
Yes |
|
No |
|
|
|||||||||||||
If yes, indicate limitations below: |
|
|
|
|
|
|
If yes, indicate limitations below: |
|
|
|
|
|
|
||||||||||||
Gender: |
Male Only |
Female Only |
N/A |
|
|
Gender: |
Male Only |
Female Only |
N/A |
|
|
||||||||||||||
Patient Age Limitation (List Ages): |
|
|
|
N/A |
|
|
Patient Age Limitation (List Ages): |
|
|
|
N/A |
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
List Other Limitations: |
|
|
|
|
|
|
List Other Limitations: |
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
Do |
|
|
|
|
|
Do |
|
|
|
|
|
||||||||||||||
practitioners, physician assistants, midwives, |
|
|
|
|
|
practitioners, physician assistants, midwives, |
|
|
|
|
|
||||||||||||||
social workers or other |
|
|
|
|
social workers or other |
|
|
|
|
||||||||||||||||
care for patients in your practice? |
|
|
|
Yes |
No |
care for patients in your practice? |
|
|
|
Yes |
No |
||||||||||||||
If yes, provide the following information for each staff member: |
If yes, indicate limitations below: |
|
|
|
|
|
|
||||||||||||||||||
|
Name: |
|
|
|
|
|
|
|
|
|
|
|
Name: |
|
|
|
|
|
|
|
|
|
|
||
|
Professional Designation: |
|
|
|
|
|
|
|
|
Professional Designation: |
|
|
|
|
|
|
|
||||||||
|
State License Number: |
|
|
|
|
|
|
|
State License Number: |
|
|
|
|
|
|
||||||||||
|
Name: |
|
|
|
|
|
|
|
|
|
|
|
Name: |
|
|
|
|
|
|
|
|
|
|
||
|
Professional Designation: |
|
|
|
|
|
|
|
|
Professional Designation: |
|
|
|
|
|
|
|
||||||||
|
State License Number: |
|
|
|
|
|
|
|
State License Number: |
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
||||||||||||||||||
|
Please attach a list of any additional |
|
Please attach a list of any additional |
||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
by health care professional: |
|
|
|
|
|
|
|
by health care professional: |
|
|
|
|
|
|
||||||||||
|
by office personnel: |
|
|
|
|
|
|
|
|
by office personnel: |
|
|
|
|
|
|
|
||||||||
Are interpreters available? |
Yes |
No |
|
|
|
Are interpreters available? |
Yes |
No |
|
|
|
||||||||||||||
If yes, specify languages: |
|
|
|
|
|
|
If yes, specify languages: |
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
Does this office meet ADA |
|
|
|
|
|
|
Does this office meet ADA |
|
|
|
|
|
|
||||||||||||
accessibility standards? |
Yes |
|
|
No |
|
|
accessibility standards? |
Yes |
|
|
No |
|
|
||||||||||||
|
|
|
|
||||||||||||||||||||||
Does this site provide handicapped accessibility for each of the |
Does this site provide handicapped accessibility for each of the |
||||||||||||||||||||||||
following: |
|
|
|
|
|
|
|
|
|
following: |
|
|
|
|
|
|
|
|
|
||||||
|
Building |
|
|
|
Yes |
|
|
No |
|
|
|
Building |
|
|
|
Yes |
|
No |
|
|
|||||
|
Parking |
|
|
|
Yes |
|
|
No |
|
|
|
Parking |
|
|
|
Yes |
|
No |
|
|
|||||
|
Restroom |
|
|
|
Yes |
|
|
No |
|
|
|
Restroom |
|
|
|
Yes |
|
No |
|
|
|||||
|
Other: |
|
|
|
|
|
|
|
|
|
|
|
Other: |
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|||||||||||||||||||
Does this site have other services for the disabled? |
|
|
Does this site have other services for the disabled? |
|
|
|
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
Yes |
No |
|
|
|
|
|
|
|
|
|
Yes |
|
No |
|||
If yes, indicate type: |
|
|
|
|
|
|
|
|
|
If yes, indicate type: |
|
|
|
|
|
|
|
|
|
||||||
|
Text Telephony - TTY |
|
|
Yes |
No |
|
Text Telephony - TTY |
|
|
Yes |
|
No |
|||||||||||||
|
American Sign |
|
|
Yes |
No |
|
American Sign |
|
|
Yes |
|
No |
|||||||||||||
|
Mental/Physical Impairment Services |
|
Yes |
No |
|
Mental/Physical Impairment Services |
|
Yes |
|
No |
|||||||||||||||
|
Other: |
|
|
|
|
|
|
|
|
|
|
Other: |
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(Continue on next page.)
|
|
DEC 05 |
Page 7 of 14 Pages. |
NEW JERSEY UNIVERSAL PHYSICIAN APPLICATION (Continued)
Other Practice Information (specify for each site)
(Continued from previous page.)
|
|
|
|
Site 1, Continued |
|
|
|
|
|
|
|
|
Site 2, Continued |
|
|
|
|
||
|
Is this site accessible by public transportation? |
|
|
|
|
|
Is this site accessible by public transportation? |
|
|
|
|
||||||||
|
|
|
|
|
Yes |
No |
|
|
|
|
|
|
|
Yes |
No |
|
|
||
|
|
Bus |
Yes |
No |
|
|
|
|
Bus |
Yes |
No |
|
|
||||||
|
|
Subway |
Yes |
No |
|
|
|
|
Subway |
Yes |
No |
|
|
||||||
|
|
Regional Train |
Yes |
No |
|
|
|
|
Regional Train |
Yes |
No |
|
|
||||||
|
|
Other: |
|
|
|
|
|
|
|
|
Other: |
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
Does this site provide childcare services? |
Yes |
No |
|
Does this site provide childcare services? |
Yes |
No |
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
Does this office qualify |
|
|
|
|
|
|
Does this office qualify |
|
|
|
|
|
||||||
|
as a minority business enterprise? |
|
Yes |
No |
|
as a minority business enterprise? |
|
Yes |
No |
||||||||||
|
Do you or does someone in your office have the following |
|
|
|
Do you or does someone in your office have the following |
|
|
||||||||||||
|
certifications? (Indicate for each office location.) |
|
|
|
|
|
certifications? (Indicate for each office location.) |
|
|
||||||||||
|
|
|
|
|
Yes |
No Exp.Date |
|
|
|
|
|
Yes |
No Exp.Date |
||||||
|
BLS (Basic Life Support) |
|
|
|
|
|
|
BLS (Basic Life Support) |
|
|
|
|
|
||||||
|
ACLS (Advanced Cardiac Life Support) |
|
|
|
|
|
ACLS (Advanced Cardiac Life Support) |
|
|
|
|
||||||||
|
ALSO (Advanced Life Support in OB) |
|
|
|
|
|
ALSO (Advanced Life Support in OB) |
|
|
|
|
||||||||
|
PALS (Pediatric Advanced Life Support) |
|
|
|
|
|
PALS (Pediatric Advanced Life Support) |
|
|
|
|
||||||||
|
ATLS (Advanced Trauma Life Support) |
|
|
|
|
|
ATLS (Advanced Trauma Life Support) |
|
|
|
|
||||||||
|
NALS (Neonatal Advanced Life Support) |
|
|
|
|
|
NALS (Neonatal Advanced Life Support) |
|
|
|
|
||||||||
|
CPR |
|
|
|
|
|
CPR |
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
||||||||||||
|
Does your site provide any of the following services on site? |
|
Does your site provide any of the following services on site? |
||||||||||||||||
|
(Indicate for each office location.) |
|
|
|
|
|
|
(Indicate for each office location.) |
|
|
|
|
|
||||||
|
Laboratory Services |
|
Yes |
No |
|
Laboratory Services |
|
Yes |
No |
||||||||||
|
Certificate of Participation from CLIA or |
|
|
|
|
|
Certificate of Participation from CLIA or |
|
|
|
|
||||||||
|
another accrediting/certifying program |
|
|
|
|
|
another accrediting/certifying program |
|
|
|
|
||||||||
|
[AAFP, COLA, CAP, Medical Laboratory |
|
|
|
|
|
[AAFP, COLA, CAP, Medical Laboratory |
|
|
|
|
||||||||
|
Evaluation (MLE)] Program |
|
Yes |
No |
|
Evaluation (MLE)] Program |
|
Yes |
No |
||||||||||
|
If yes, list program: |
|
|
|
|
|
|
|
If yes, list program: |
|
|
|
|
|
|
||||
|
Radiology Services |
|
Yes |
No |
|
Radiology Services |
|
Yes |
No |
||||||||||
|
|
Yes |
No |
|
|
Yes |
No |
||||||||||||
|
If yes, include type: |
|
|
|
|
|
|
|
If yes, include type: |
|
|
|
|
|
|
||||
|
EKG’s |
|
Yes |
No |
|
EKG’s |
|
Yes |
No |
||||||||||
|
Care of Minor Lacerations |
|
Yes |
No |
|
Care of Minor Lacerations |
|
Yes |
No |
||||||||||
|
Pulmonary Function Testing |
|
Yes |
No |
|
Pulmonary Function Testing |
|
Yes |
No |
||||||||||
|
Allergy Injections |
|
Yes |
No |
|
Allergy Injections |
|
Yes |
No |
||||||||||
|
Allergy Skin Testing |
|
Yes |
No |
|
Allergy Skin Testing |
|
Yes |
No |
||||||||||
|
Office Gynecology (Routine Pelvic/Pap) |
Yes |
No |
|
Office Gynecology (Routine Pelvic/Pap) |
Yes |
No |
||||||||||||
|
Drawing Blood |
|
Yes |
No |
|
Drawing Blood |
|
Yes |
No |
||||||||||
|
Age Appropriate Immunizations |
|
Yes |
No |
|
Age Appropriate Immunizations |
|
Yes |
No |
||||||||||
|
Flexible Sigmoidoscopy |
|
Yes |
No |
|
Flexible Sigmoidoscopy |
|
Yes |
No |
||||||||||
|
Tympanometry/Audiometry Screening |
Yes |
No |
|
Tympanometry/Audiometry Screening |
Yes |
No |
||||||||||||
|
Asthma Treatment |
|
Yes |
No |
|
Asthma Treatment |
|
Yes |
No |
||||||||||
|
Osteopathic Manipulation |
|
Yes |
No |
|
Osteopathic Manipulation |
|
Yes |
No |
||||||||||
|
IV Hydration/Treatment |
|
Yes |
No |
|
IV Hydration/Treatment |
|
Yes |
No |
||||||||||
|
Cardiac Stress Tests |
|
Yes |
No |
|
Cardiac Stress Tests |
|
Yes |
No |
||||||||||
|
Physical Therapy |
|
Yes |
No |
|
Physical Therapy |
|
Yes |
No |
||||||||||
|
|
|
|
|
|
||||||||||||||
|
Additional Office Procedures Provided (incl. surgical procedures) |
|
Additional Office Procedures Provided (incl. surgical procedures) |
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
||||||||||
|
Is anesthesia administered in your office? |
Yes |
No |
|
Is anesthesia administered in your office? |
Yes |
No |
||||||||||||
|
If Yes, what class or category of anesthesia do you use? |
|
|
|
If Yes, what class or category of anesthesia do you use? |
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
Who administers it? |
|
|
|
|
|
|
Who administers it? |
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
For additional office sites, please submit an attachment containing the above information and check this box:
|
|
DEC 05 |
Page 8 of 14 Pages. |
NEW JERSEY UNIVERSAL PHYSICIAN APPLICATION (Continued)
Patient Scheduling
What is patient wait time for emergency care? .................................................
What is patient wait time for urgent care?.........................................................
What is patient wait time for symptomatic care?...............................................
What is patient wait time for scheduling routine visits? .....................................
What is patient wait time for scheduling routine care? ......................................
What is average wait time for patients between waiting room and examination?
What is average wait time in minutes for returning a patient’s call?..................
Required Attachments or Supplemental Information
Please attach hard copy or scanned documents of the following:
♦Copy(ies) of DEA registration certificate(s)
♦Copy of state Controlled Dangerous Substance (CDS) registration certificate(s)
♦Copy of current professional liability insurance policy face sheet, showing expiration dates, limits and provider’s name
♦Copy(ies) of
♦Copy of workers compensation certificate of coverage, if applicable
SECTION 2 - DISCLOSURE QUESTIONS
Please answer each question and include an explanation for any question answered “Yes.”
Licensure
1.Has your license to practice, in your profession, ever been denied, suspended, revoked, restricted, voluntarily surrendered while under investigation or have you ever been subject to
a consent order, probation or any conditions or limitations by any state licensing board?...................
2.Have you ever received a reprimand or been fined by any state licensing board?..............................
Yes
Yes
No No
Hospital Privileges and Other Affiliations
3.Have your clinical privileges at any hospital or healthcare institution ever been denied, suspended, revoked, restricted, denied renewal or subject to probationary or to other disciplinary conditions (for reasons other than
4.Have you voluntarily surrendered, limited your privileges or not reapplied for privileges while under investigation?.............................................................................................................................
5.Have you ever been terminated for cause or not renewed for cause from participation, or been subject to any disciplinary action, by any managed care organizations (including HMOs, PPOs, or provider organizations such as IPAs, PHOs)? .....................................................................
Yes
Yes
Yes
No
No
No
Education, Training and Board Certification
6.Were you ever placed on probation, disciplined, formally reprimanded, suspended or asked to resign during an internship, residency, fellowship, preceptorship or other clinical education program? If you are currently in a training program, have you been placed on probation, disciplined, formally reprimanded, suspended or asked to resign? .....................................................
7.Have you ever, while under investigation, voluntarily withdrawn or prematurely terminated your status as a student or employee in any internship, residency, fellowship, preceptorship,
or other clinical education program?....................................................................................................
8.Have any of your board certifications or eligibility ever been revoked? ...............................................
9.Have you ever chosen not to
Yes
Yes
Yes
Yes
No
No No
No
|
|
DEC 05 |
Page 9 of 14 Pages. |
NEW JERSEY UNIVERSAL PHYSICIAN APPLICATION (Continued)
DEA or CDS Certification/Authorization
10.Have your Federal DEA and/or State Controlled Dangerous Substances (CDS) certificate(s)
or authorization(s) ever been denied, suspended, revoked, restricted, denied renewal, or |
|
|
voluntarily relinquished? |
Yes |
No |
Medicare, Medicaid or Other Governmental Program Participation
11.Have you ever been disciplined, excluded from, debarred, suspended, reprimanded, sanctioned, censured, disqualified, subject to a recovery action or otherwise restricted in
regard to participation in the Medicare or Medicaid program, or in regard to other federal or |
|
|
state governmental health care plans or programs? |
Yes |
No |
Other Sanctions or Investigations
12.Are you currently or have you ever been the subject of an investigation by any hospital, licensing authority, DEA or CDS authorizing entities, education or training program, Medicare
or Medicaid program, or any other private, federal or state health program? ......................................
13.To your knowledge, has information pertaining to you ever been reported to the National Practitioner Data Bank or Healthcare Integrity and Protection Data Bank?.........................................
14.Have you ever received sanctions from or been the subject of investigation by any regulatory agencies (e.g., CLIA, OSHA, etc.)? ....................................................................................................
15.Has a patient, employee, or
16.Have you ever been investigated, sanctioned, reprimanded or cautioned by a military hospital, facility, or agency, or voluntarily terminated or resigned while under investigation by
a hospital or healthcare facility of any military agency? .......................................................................
Yes
Yes
Yes
Yes
Yes
No
No
No
No
No
Professional Liability Insurance Information and Claims History
17.Has your professional liability coverage ever been cancelled, restricted, declined or not renewed by the carrier based on your individual liability history? ........................................................
18.Have you ever been assessed a surcharge, or rated in a
your professional liability insurance carrier, based on your individual liability history? ........................
Yes
Yes
No
No
Malpractice Claims History
19.Have you ever had any malpractice actions (pending, settled, dropped, dismissed, arbitrated, mediated or litigated)? If yes, provide information for each case on the attached form located
at the end of the Disclosure questions (list all separately)...................................................................
For any malpractice actions, please complete addendum and check this box:
Yes
No
Criminal/Civil History
(Note: A criminal record will not necessarily be a bar to acceptance. Decisions will be made by each health plan or credentialing organization based upon all relevant circumstances, including the nature of the crime.)
20.Have you ever been arrested, charged or indicted for, convicted of, pled guilty to, or pled nolo contendere to any felony, crime or other offense in the last ten years or been found liable or responsible for or named as a defendant in any civil offense that is reasonably related to your qualifications, competence, functions, or duties as a medical professional? ...............
21.Have you ever been arrested, charged or indicted for, convicted of, pled guilty to, or pled nolo contendere to any felony, crime or other offense in the last ten years or been found liable or responsible for or been named as a defendant in any civil offense that alleged fraud,
an act of violence, child abuse or a sexual offense or sexual misconduct?.........................................
22.Have you ever been
Yes
Yes
Yes
No
No
No
|
|
DEC 05 |
Page 10 of 14 Pages. |
Document Specifications
| Fact Name | Detail |
|---|---|
| Personal Information Requirement | The New Jersey Universal Physician Application requires comprehensive personal information, including the physician's name, degrees, social security number, date of birth, and gender. Additionally, it inquires regarding eligibility to work in the United States. |
| Practice Location Information | Physicians must provide detailed information about their practice location(s), including type of service provided, name of the physician group/practice, mailing address, contact numbers, tax ID, and whether the site should be listed in the directory. |
| Professional Licensing and Certification | Applicants are required to list all medical licenses and certifications, including the state of licensure, license numbers, expiration dates, and details on DEA and CDS registration certificates. It also asks about Medicare and Medicaid Provider participations. |
| Professional Liability Insurance Coverage | The form requests information on the physician's current malpractice insurance carrier, policy number, effective and expiration dates, coverage amounts, and type of coverage. It also inquires about any interests in outside clinical labs. |
Detailed Steps for Using Nj Universal Physician Application
Filling out the New Jersey Universal Physician Application is a crucial step for physicians seeking to establish or continue their practice within the state. This comprehensive document collects detailed information about a physician's personal details, educational background, professional training, certifications, and work history, among other critical data. Completing the application accurately is vital for ensuring smooth processing and validation of one's professional credentials. Here is a step-by-step guide to assist in filling out this application:
- Begin with SECTION 1: Personal Information. Type or print your full name, including any suffixes (Jr., Sr., etc.), professional degrees, social security number, any former names and the duration those were used, date of birth, gender, and work eligibility in the United States.
- Fill in your home mailing address including city, state, and zip code.
- Under Practice Location Information, indicate the type of service provided (Primary Care Specialist, Non-Primary Care Specialist), the practice name to appear in the directory, and if applicable, a different group or corporate name for W-9 purposes. Include the primary office's mailing address, phone number, fax number, and email address.
- For Tax ID Number and associated group number and name for your location, provide the required details. Indicate if you are currently practicing at this address and if you wish to list this site in the directory.
- Repeat the above step for any other office locations and indicate whether you want these sites listed in the Directory.
- Proceed to License and Other Identification Numbers. Include all relevant licensures and certifications, specifying the state, license/certificate numbers, expiration dates, and if you currently practice under these licenses.
- For DEA and CDS Registration Certificates, fill in the respective details.
- Indicate if you are a participating Medicare and/or Medicaid provider.
- If an International Medical Graduate, provide your ECFMG certification number and issue date.
- Under Medical Education, list your degree-issuing institution and attendance dates. If you attended additional schools, note this and attach supplemental information.
- Detail your Post-Graduate Education including internships, fellowships, residencies, and any teaching appointments.
- In the Professional/Medical Specialty Information section, specify your primary and if applicable, secondary specialties, including certification statuses and certifying boards.
- List any additional areas of professional practice, interest, or focus.
- Provide information on your hospital privileges and affiliations, specifying types of privileges and percentages of total admissions per hospital.
- Include a complete Work History since completion of training, and explain any gaps greater than six months.
- List three professional references, ensuring they are not partners in your practice or relatives.
- For Professional Liability Insurance Coverage, specify whether you are self-insured and provide details of your current and previous malpractice insurance or self-insured entities.
- Indicate your status/role in practice and any interests in outside clinical labs, providing legal billing name and description.
- List names of colleagues providing office coverage, including their specialties.
- If applicable, list full names of all partners in your practice.
Upon completing the form, review all information for accuracy before submission. Ensure any additional required documents or attachments are included as specified throughout the application. This careful attention to detail will facilitate a smoother review process and contribute to a successful application outcome.
Learn More on Nj Universal Physician Application
What is the New Jersey Universal Physician Application?
The New Jersey Universal Physician Application is a comprehensive form designed for physicians who wish to apply for medical credentialing in the state of New Jersey. It collects detailed personal and professional information, including but not limited to personal details, practice location information, license and identification numbers, medical education, professional or medical specialty information, hospital affiliations and privileges, work history, references, and professional liability insurance coverage. The form serves as a universal application, making it easier for physicians to submit their information for various credentialing purposes within the state.
Who needs to complete the New Jersey Universal Physician Application?
Any physician seeking medical credentialing in New Jersey needs to complete the New Jersey Universal Physician Application. This includes both new applicants applying for the first time and existing practitioners who are renewing or updating their credentials. This comprehensive form is also applicable to physicians who may be changing their practice location, updating their specialty or hospital affiliations, or have had any significant changes in their work history or professional liability insurance coverage.
What information is required when completing the application?
The application requires a range of detailed information that includes:
- Personal Information: Such as name, social security number, date of birth, and eligibility to work in the U.S.
- Practice Location Information: Details about the primary and, if applicable, other practice locations.
- License and Other Identification Numbers: Including all license(s) and certifications in all states where the physician is currently or has previously been licensed, as well as DEA and CDS registration certificates.
- Medical Education and Post-Graduate Education: Schools attended, degrees earned, and any post-graduate education.
- Professional/Medical Specialty Information: Primary specialty, board certification details, and any secondary or additional specialties.
- Hospital Affiliations and Privileges: Information about current hospital privileges and any previous affiliations.
- Work History: A chronological summary of work history since completion of training along with explanations for any gaps.
- References: Details of three professional references.
- Professional Liability Insurance Coverage: Information regarding current and previous malpractice insurance coverage.
How do I submit the New Jersey Universal Physician Application?
After completing the New Jersey Universal Physician Application, the form should be reviewed to ensure all information is accurate and complete. Any additional documentation required, such as attachments detailing further medical education, additional hospital affiliations, or extended work history, should be included with the application. The completed form, along with all necessary attachments, should be submitted to the relevant credentialing board or authority as indicated in the application instructions. It's advisable to keep a copy of the full application and all documents for your records.
Common mistakes
When completing the New Jersey Universal Physician Application, applicants commonly make several avoidable errors. Identifying and rectifying these mistakes is crucial for a seamless application process. Here are five common mistakes:
- Incorrectly entering personal information: Applicants often misspell their names, use nicknames instead of legal names, or enter incorrect Social Security Numbers. This leads to delays in the processing of the application.
- Omitting former names: Failing to list all former names, including maiden and previously legally changed names, linked with specific years can cause verification issues.
- Incomplete education and training sections: Not providing complete details about medical education, including attendance dates and addresses, or failing to attach additional pages for multiple schools or training programs.
- Licensing and certification details: Applicants sometimes forget to include information about all licenses and certifications held in other states or fail to update them with current expiration dates. Some also neglect to specify whether they are currently practicing in each state listed.
- Work history gaps: Not explaining gaps of six months or more in the work history section. This can raise questions about the applicant's professional journey and delay the application process.
To avoid these mistakes, applicants are encouraged to review their applications carefully and ensure accuracy and completeness in every section. This diligence will help streamline the credentialing process and avoid unnecessary delays.
Documents used along the form
The New Jersey Universal Physician Application is a comprehensive form designed to streamline the credentialing and application process for physicians in New Jersey. It gathers personal, educational, and professional details of a physician seeking licensure or privileges in the state. To present a complete profile and ensure compliance with regulatory requirements, applicants often need to supplement this form with additional documents. These documents not only validate the information provided but also offer a deeper insight into the physician's qualifications, competencies, and legal standing.
- Certificate of Medical Education: This certificate provides verification of the applicant’s graduation from an accredited medical school. It is essential for confirming the authenticity of the medical degree listed on the New Jersey Universal Physician Application.
- Board Certification Documents: These documents serve as proof that the applicant has met specialized standards in their field of medicine, beyond the basic medical licensure. They indicate whether a physician is board certified and detail the specialty or specialties in which the physician is certified.
- Malpractice Insurance Certificate: This document is proof of the physician's current professional liability insurance coverage. It must detail the policy number, coverage amounts per occurrence and in aggregate, effective and expiration dates, and the insurance carrier's contact information.
- Continuing Medical Education (CME) Certificates: CME certificates demonstrate that the physician has engaged in ongoing education to maintain, develop, or increase the knowledge, skills, and professional performance needed to provide services for patients, the public, or the profession. They are critical for ensuring the physician's knowledge is current.
- Letter of Recommendation: Typically, several letters from colleagues or healthcare professionals who can attest to the applicant's clinical skills, professionalism, and suitability for practice. Although not always mandatory, they can significantly support an application, especially in competitive specialties or sought-after hospitals.
Together, the New Jersey Universal Physician Application and these supplementary documents provide a robust framework for evaluating a physician's eligibility and qualifications. The process ensures that only qualified individuals are granted licensure or privileges, thereby maintaining high standards of medical practice within New Jersey.
Similar forms
The New Jersey Universal Physician Application form bears a resemblance to the Medical Staff Credentialing Application forms used by hospitals and health systems for granting medical staff privileges. Both documents collect detailed personal, educational, and professional information from physicians, including work history, medical education, and licenship details. The goal is to verify the qualifications and competency of the applying physicians to ensure that they meet the specific credentialing standards of the facility.
A Physicians' State License Application is another document with similarities to the New Jersey Universal Physician Application form. Both require detailed information about the physician's education, training, and current licensure status. State license applications ensure that physicians meet the state's regulatory requirements to practice medicine, while the Universal Application also includes data relevant to employment and hospital privileges.
The Drug Enforcement Administration (DEA) Registration Form for prescribers is similarly detailed, asking for information about licensure, educational background, and practice locations. Like the New Jersey Universal Physician Application, the DEA form is required for physicians to legally prescribe controlled substances. Both forms play a critical role in the regulatory oversight of medical professionals to ensure public safety.
The Curriculum Vitae (CV) of a physician shares the purpose of detailing a doctor's education, training, and professional experiences like the New Jersey Universal Physician Application. While the Universal Application is a standardized form for employment and credentialing purposes, a CV offers a more personal narrative of a physician's career journey, including publications and research interests.
Professional Liability Insurance Applications resemble the New Jersey Universal Physician Application in that they require comprehensive professional information. Both documents need details on the physician's education, practice location, and work history to assess eligibility and risk for insurance coverage. This ensures that physicians are adequately protected against claims of professional negligence.
Board Certification Applications for medical specialties request extensive details about a physician's education, training, and expertise, akin to the Universal Physician Application. Both forms are essential for validating the physician's qualifications in their field, albeit for different reasons; one for credentialing within a healthcare setting and the other for recognition by a specialty board.
The Medicare and Medicaid Provider Enrollment Applications, much like the New Jersey Universal Physician Application, collect detailed personal and professional information to ensure compliance with federal and state healthcare program standards. These applications play an essential role in the healthcare reimbursement process, determining the physician's eligibility to receive payments from these programs.
Physician Employment Applications, often utilized by healthcare organizations during the hiring process, share characteristics with the Universal Physician Philip Application. They gather data on education, training, licensure, and work history to assess a candidate's suitability for a position, focusing on understanding the professional credentials and experience of the applicant.
Fellowship and Residency Program Applications also mirror the Universal Physician Application in the necessity to detail a doctor's educational background, training, and areas of specialty. These forms are an essential step in a physician's career, allowing them to continue their education in a specific field of medicine, ensuring they have the requisite knowledge and skills.
Finally, Continuing Medical Education (CME) Credit Reporting Forms resemble the New Jersey Universal Physician Application by requiring doctors to document their ongoing educational activities. Both types of documents serve to ensure that physicians remain up-to-date with the latest knowledge and practices in their field, maintaining high standards of patient care.
Dos and Don'ts
When completing the New Jersey Universal Physician Application form, it's crucial to pay close attention to every detail to ensure the accuracy and completeness of the application. Here are some dos and don'ts to keep in mind:
- Do ensure all information is legible. Whether typing or printing, clarity is key. This prevents any misunderstandings or delays in processing your application.
- Don't rush through the form. Take your time to read and understand each section to avoid making errors. Incomplete or incorrect submissions can lead to delays.
- Do verify your information before submitting. Double-check your entries, especially critical details like license numbers, SSN, and contact information.
- Don't leave any fields blank unless specified. If a section doesn’t apply to you, consider marking it as “N/A” to indicate that you have reviewed the section.
- Do use additional sheets if necessary. If you have more information than the form allows (e.g., previous hospital affiliations or work history), attach additional pages as instructed, making sure they are clearly marked and attached securely.
- Don't forget to sign and date the application. An unsigned application is incomplete. Ensure you also check any certification or acknowledgment sections that require your attention.
- Do keep a copy for your records. Before submitting the application, make a copy for your personal files. This will be helpful for your records and in case the original is lost.
- Don't include sensitive information via insecure channels. If you're submitting additional documents or clarifications via email or other digital means, ensure the method is secure to protect your personal and professional information.
Adhering to these guidelines will streamline the application process, helping to avoid common pitfalls that can delay your ability to practice within New Jersey. It’s in the interest of an applicant to meticulously review their submission, ensuring it reflects their qualifications and complies with the requirements set out by the State.
Misconceptions
- One common misconception is that the New Jersey Universal Physician Application only applies to physicians currently practicing in New Jersey. In reality, the form is also relevant for physicians planning to start practice in the state, as indicated by the option to provide an expected start date if not currently practicing at a given location.
- Many believe that only primary care physicians need to complete the application. However, the form clearly accommodates specialists and non-primary care specialists, asking applicants to specify their type of service provided.
- Another misconception is that the application form is solely for individual physicians. While it's tailored to individual providers, it requests information about group practices, indicating that it's also relevant for physicians associated with groups or corporate entities.
- There's a mistaken belief that the application doesn't cover medical education or training outside the United States. The section for International Medical Graduates and the option to list additional schools attended underscore its comprehensive nature, encompassing both domestic and international training.
- Some think the form exclusively deals with current licensing and certification. Yet, it seeks details on past licenses and certifications across different states, not just current statuses, highlighting a broader scope that covers a physician's entire licensing history.
- A final misconception is that the application overlooks professional liability insurance. On the contrary, there are specific sections dedicated to both current and previous malpractice insurance, debunking the idea that it only focuses on practice and credentials without considering insurance coverage.
Key takeaways
Filling out the New Jersey Universal Physician Application is a necessary step for physicians planning to practice in New Jersey. Whether you're a new doctor in the state or an experienced physician updating your credentials, understanding the key components of this form is essential. Here are four important takeaways to keep in mind:
- Complete Personal and Professional Information: The form requires comprehensive details starting with personal information such as your name, Social Security number, and contact details. Professional information includes your degrees, practice locations, type of service provided, and tax ID numbers for each location. It's crucial to ensure all information is accurate and up to date.
- Licensing and Certification Details: You must include all your licensing information, whether you're currently practicing in New Jersey or in other states. This encompasses license numbers, expiration dates, and any certifications from medical boards. For international medical graduates, certification by the Educational Council for Foreign Medical Graduates (ECFMG) is also required.
- Education and Work History: The application asks for a detailed account of your medical education, post-graduate education, and any additional graduate-level education. Furthermore, providing a complete chronological work history since the completion of your training is necessary to account for your professional experience.
- Professional Liability Insurance Coverage: Physicians must disclose their current malpractice insurance carrier, policy numbers, coverage amounts, and the effective dates of their policies. Details regarding any previous malpractice insurance carriers are also required to ensure there are no gaps in coverage.
By keeping these key points in mind and accurately reporting the required information, physicians can ensure a smoother application process. This comprehensive approach helps in avoiding any delays or issues with credentialing and licensing in New Jersey. Don't forget to check for any attachments you may need to include for additional offices, education, or work history to provide a full representation of your professional profile.
Popular PDF Documents
Nj Resale Certificate - Before using the ST-7 form, farmers must verify their eligibility as not all agricultural activities qualify for this exemption.
Nj Reg - Entities engaging in selling, storing, or delivering petroleum products in New Jersey need to report these activities via the NJ-REG form.